US Pharm. 2008;33(10):46-51.
Long before there were
antibiotics, researchers envisioned using viruses to seek out and destroy
bacteria. Now, as organisms continue to develop resistance to existing
antibiotics, these viruses, called bacteriophages, are finding new
advocates. According to the FDA, bacteriophages (or phages) are defined
as RNA or DNA viruses that infect bacteria without infecting mammalian or
plant cells. Phages are ubiquitous in the environment, and humans are
routinely exposed to them at high levels through food and water without
adverse effects. The FDA has approved one product, a Listeria-specific
bacteriophage preparation made from six individually purified phages to be
used on ready-to-eat meat and dairy products, as an antimicrobial agent.1
The product, a food additive, is reported to be effective against 170 strains
of Listeria monocytogenes. Other phages have been approved in the
United States as pesticides.
Although not currently
permitted here, phages are used abroad (e.g., in Eastern Europe, the former
Soviet Union) as antibiotic therapy. Phages may eventually become the
treatment of choice in the U.S. for cases where antibiotics fail, but there
are a host of problems to be solved before that happens. This article will
review the history of phage discovery, biology, medical uses, advantages and
disadvantages, and the likely future of phage therapy.
History
A paper written by
Frederick Twort and published in 1915 is generally considered the beginning of
phage research, although there are earlier reports that suggest their presence.2
Twort was attempting to grow vaccinia virus on agar media in the absence of
living cells when he noted that some colonies of contaminating micrococci
appeared mucoid, watery, or glassy. This glassy transformation could be
induced in other colonies by inoculation of the fresh colony with material
from the watery colony. When he examined the glassy colonies under a
microscope, he noted that the bacteria had degenerated into small granules.
His interpretation of glassy transformation was tentative, but he concluded
that the agent responsible might almost be considered as an acute infectious
disease of micrococci.3
Although he may not have been
first to publish, Felix d'Herelle is generally credited as the scientist most
intimately involved in phage research and its medical application.4
The discovery or rediscovery of phages by d'Herelle is associated with an
outbreak of severe hemorrhagic dysentery among French troops stationed on the
outskirts of Paris in 1915. Several soldiers were hospitalized, and d'Herelle
was assigned to conduct an investigation of the outbreak. During these
studies, he made bacteria-free filtrates of the patients' fecal samples and
mixed and incubated them with Shigella strains isolated from the
patients. A portion of the mixtures was inoculated into experimental animals
and a portion was spread on agar medium to observe the growth of the bacteria.
It was on these agar cultures that d'Herelle observed the appearance of small,
clear areas, which he initially called taches, and later plaques.5
His findings were presented during the September 1917 meeting of the Academy
of Sciences, and they were subsequently published in the meeting's proceedings.6
D'Herelle had little doubt about the nature of the phenomenon, and he proposed
that it was caused by a virus capable of parasitizing bacteria. He also
proposed the name bacteriophage on October 18, 1916.7 The
name was formed from bacteria and phagein (Greek, "to eat or
devour") to imply that phages consume or destroy bacteria.
Biology
As mentioned
earlier, phages are DNA or RNA viruses that infect only specific bacteria.
They have colorful names such as T4, Mu, Qfl, P1, or CTXØ.
Bacterial phages come in many shapes and sizes (e.g., tailed or nontailed,
icosahedral, filamentous, and enveloped or nonenveloped). The tailed,
double-stranded DNA phages began evolving over three billion years ago, but
only in recent years has science begun to understand the genetic mechanisms
behind that evolution and the role they play in the evolution of their
bacterial hosts. It has also become clear that not only are tailed phages
remarkably abundant in the environment, but they also probably constitute a
numerical majority of organisms on the planet.8 Estimates of the
total population are on the order of 1031 total viral particles, an
astronomical number: 1031 tailed phages laid end to end would
extend into space to a distance of 200 million light years. Estimates of the
longevity of phages in the environment suggest that the entire population
turns over every few days.9
Phages can assume many
different lifestyles--lytic or temperate. Lytic phages infect a
bacterium and immediately begin replicating, destroying the cell a short time
later.9 Temperate phages can arm a bacterium with an
additional poisonous gene and turn it into a lethal weapon.4 They
also integrate their DNA into the bacterial chromosome, leading to a state of
lysogeny. (A phage in the lysogenic state is called a prophage.)
Certain prophages can alter the phenotype of the host bacterium. If the
prophage expresses a toxin gene, then the bacterium will be lysogenically
converted for toxin production. For example, the virulence of Vibrio
cholerae is largely dependent on infection by the bacteriophage CTXØ,
in that the cholera toxin is
encoded within the genome of this temperate and nonlytic filamentous phage,
and only strains of vibrio infected by CTXØ are
capable of causing epidemic disease.9
Most phages have
double-stranded DNAs encapsulated into an icosahedral shell of protein
attached to a tail. At the end of the tail there are proteins that attach to
cells. A simple explanation is as follows: the virus particle with its protein
and DNA first lands on the outside of the specific bacterial cell and injects
its DNA into the cell. The DNA of the bacterial virus then takes over the
cell, converting the cell into a virus factory. The bacterial cell dies, and
hundreds of virus particles are released. The process, of course, is much more
complex, consisting of a cascade of events involving several structural and
regulatory genes.
Medical Uses
Not long after his
discovery, d'Herelle used phages to treat dysentery. The studies were
conducted in Paris in 1919. The phage preparation was ingested by d'Herelle,
the treating physician, and several hospital interns to confirm its safety
before administering it to patients.7 The successful results of
these studies, however, were not immediately published, and therefore the
first reported application of phages to treat infectious diseases of humans
came from Bruynoghe and Maisin in France in 1921. They used phages to treat
staphylococcal skin disease.10
Several promising studies
followed, and encouraged by these early results, d'Herelle used various phage
preparations to treat thousands of patients having cholera and/or bubonic
plague in India. D'Herelle
also owned a commercial laboratory in Paris that produced several phage
preparations against various bacterial infections.
In the early 1930s, at least
four major manufacturers in the U.S. manufactured and sold phage products,
including Parke Davis, E. R. Squibb and Sons, Swan-Myers of Abbott
Laboratories, and Eli Lilly. All four suppliers focused primarily on
staphylococci phages, which were administered to treat furuncles, carbuncles,
and boils.4 As late as the 1940s, Eli Lilly was producing seven
phage products for human use, including preparations targeted against
staphylococci, streptococci, E. coli, and other bacterial pathogens.
These preparations consisted of phage-lysed, bacteriologically sterile broth
cultures of the targeted bacteria, or the same preparations in a water-soluble
jelly base. The products were used to treat various infections, including
abscesses, suppurating wounds, vaginitis, acute and chronic infections of the
upper respiratory tract, and mastoid infections.7
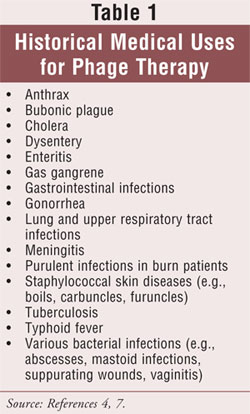
In addition to these uses,
phages have also been used to treat anthrax, enteritis caused by Campylobacter
species, Clostridium difficile gastrointestinal infections, gas
gangrene, meningitis caused by Haemophilus influenzae, lung infections
caused by Klebsiella pneumoniae, tuberculosis, gonorrhea, opportunistic
infections of the lung caused by Proteus organisms, purulent infections
related to Pseudomonas aeruginosa colonizationin burn patients, typhoid
fever, and bacterial dysentery caused by Shigella species (TABLE 1).4
Advantages and Disadvantages of
Phage Therapy
The discovery of
viruses that can infect and destroy bacteria was greeted with considerable
optimism in the early 1900s. Despite the efforts of a number of investigators,
their use was generally abandoned soon after the introduction of antibiotics
in the 1940s.11 Lytic phages, of course, are similar to antibiotics
in that they have remarkable antibacterial activity, and their theoretical
advantages are good reasons for renewed interest. Earlier reported results
using phages might have been better if it had been recognized that there are
many types of phages and that each is specific for a special host range of
bacteria. This misconception resulted in phages that were effective against
one bacterial host being applied to clinical infections caused by other
bacterial strains, against which these phages had little, if any, effect.11
Phages have a number of
advantages compared to antibiotics (TABLE 2). For one, phages are very
specific; they usually affect only the targeted bacterial species. Antibiotics
target both pathogenic microorganisms and normal microflora. This affects the
microbial balance in the patient, which may lead to a serious secondary
infection. Second, phages replicate at the site of infection and are available
where they are most needed. Antibiotics are metabolized and eliminated from
the body and do not concentrate at the site of infection. Third, phages are
found throughout nature, and it is easy to find new phages when bacteria
become resistant to them. This means that selecting new phages is a relatively
rapid process that can be accomplished in days or weeks, whereas developing a
new antibiotic is a time-consuming process that can take several years.7
Evolution drives the rapid emergence of new phages that can destroy bacteria
that have become resistant; i.e., there should be an inexhaustible supply.4
Fourth, phages appear to be safe, as no serious adverse effects have been
described. Minor adverse effects, however, have been reported due to the
liberation of endotoxins from bacteria lysed in vivo by phages.12,13
Such effects may also be observed when antibiotics are used.14
During the long history of phage usage in Eastern Europe and the former Soviet
Union, there have been virtually no reports of serious complications.7
Phages have been administered orally (tablets or liquid), rectally,
intravenously, locally, and in tampons, rinses, creams, and aerosols. Fifth,
and most important, phages are active against bacteria that have become
resistant to antibiotics.
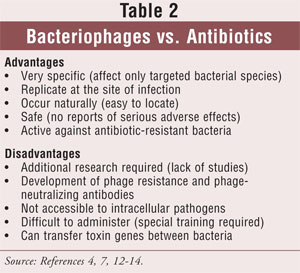
Phage therapy is not without
disadvantages (TABLE 2). There are no internationally recognized
studies that attest to the efficacy of phages in human patients. There are a
number of publications on phage therapy, but very few papers in which the
pharmacokinetics of therapeutic phage preparations is delineated.7
Additional research would be needed to obtain the type of pharmacologic and
toxicologic data required by the FDA. There is a paucity of appropriately
conducted, placebo-controlled studies. Because of the high specificity of
phages, many negative results may have been obtained because of failure to
select phages lytic for the targeted bacterial species. Another concern
regarding the therapeutic use of phages is that the development of phage
resistance may hamper their effectiveness. Because bacteria are under constant
threat of infection by phages, there are strong selective pressures to acquire
resistance. The development of phage-neutralizing antibodies is another
possible disadvantage, which may hamper phage effectiveness. It is also
unclear how effective phages would be in treating diseases caused by
intracellular pathogens (e.g., Salmonella species), where bacteria
multiply primarily inside human cells and are not accessible to phages. Phages
are more difficult to administer than antibiotics, and a physician needs
special training in order to correctly prescribe and use phages. It must also
be remembered that phages are complex organisms than can transfer toxin genes
between bacteria.4
The Future
The potential for
treating infectious diseases with phages has been pursued since their
discovery, but for the reasons outlined here, phage therapy is not accepted in
Western medicine. There still remain many important questions that must be
addressed before lytic phages can be endorsed for therapeutic use. Currently,
the FDA would have a problem approving mixtures of phages, and the agency has
yet to publish guidelines for approving phage drugs. FDA scientists have
indicated concern about phages changing during the course of manufacture, as
mutations in phage genes can have unexpected effects. However, with the
continuing threat of antibiotic resistance, it is time to reconsider
developing phage therapy to the point where it can be useful in modern
clinical practice.15 There is a sufficient body of data to build on
and a desperate need for an alternative treatment against emerging
antibiotic-resistant bacteria.
REFERENCES
1. FDA approval of
Listeria-specific bacteriophage preparation on ready-to-eat (RTE) meat and
poultry products. CFSAN/Office of Food Additive Safety. August 2006.
www.cfsan.fda.gov/~dms/opabacqa.html. Accessed August 27, 2008.
2. Summers WC. History
of phage research and phage therapy. In: Waldor MK, Friedman DI, Adhya SL,
eds. Phages: Their Role in Bacterial Pathogenesis and Biotechnology.
Washington, DC: ASM Press; 2005:3-17.
3. Twort FE. An
investigation on the nature of ultra-microscopic viruses. Lancet.
1915;2:1241-1243.
4. Hausler T. Viruses
vs. Superbugs: A Solution to the Antibiotics Crisis? London, UK:
Macmillan; 2007.
5. Summers WC. Felix
d'Herelle and the Origins of Molecular Biology. New Haven, CT: Yale
University Press; 1999.
6. D'Herelle F. Sur un
microbe invisible antagoniste des bacilles dysenteriques. CR Acad Sci.
1917;165:373-375.
7. Sulakvelidze A,
Alavidze Z, Morris JG Jr. Bacteriophage therapy. Antimicrob Agents
Chemother. 2001;45:649-659.
8. Thacker PD. Set a
microbe to kill a microbe: drug resistance renews interest in phage therapy. JAMA.
2003;290:3183-3185.
9. Hendrix RW.
Bacteriophage evolution and the role of phages in host evolution. In: Waldor
MK, Friedman DI, Adhya SL, eds. Phages: Their Role in Bacterial
Pathogenesis and Biotechnology. Washington, DC: ASM Press; 2005:55-65.
10. Bruynoghe R, Maisin
J. Essais de therapeutique au moyen du bacteriophage. CR Soc Biol.
1921;85:1120-1121.
11. Merril CR, Biswas
B, Carlton R, et al. Long-circulating bacteriophage as antibacterial agents. Proc
Natl Acad Sci USA.1996;93:3188-3192.
12. Cislo M, Dabrowski
M, Weber-Dabrowska B, Woyton A. Bacteriophage treatment of suppurative skin
infections. Arch Immunol Ther Exp (Warsz). 1987;2:175-183.
13. Slopek S,
Weber-Dabrowska B, Dabrowski M, Kucharewicz-Krukowska A. Results of
bacteriophage treatment of suppurative bacterial infections in the years
1981-1986. Arch Immunol Ther Exp (Warsz). 1987:35:569-583.
14. Prins JM, van
Deventer SJ, Kuijper EJ, Speelman P. Clinical relevance of antibiotic-induced
endotoxin release. Antimicrob Agents Chemother. 1994;38:1211-1218.
15. McKinstry M, Edgar
R. Use of phages in therapy and bacterial detection. In: Waldor MD, Friedman
DI, Adhya SL, eds. Phages: Their Role in Bacterial Pathogenesis and
Biotechnology. Washington, DC: ASM Press; 2005:430-440.
To comment on this article, contact
rdavidson@jobson.com.


