US Pharm. 2007;32(4):10.
Allergic diseases are important causes of morbidity in the United States. The National Ambulatory Medical Care Survey reported that allergic rhinitis, asthma, and contact dermatitis or eczema were among the 15 most common diagnoses made in patients 11 to 20 years old. In addition, injections of allergenic extracts were the most commonly prescribed drug in those age 11 to 14 years and the second most common in those 15 to 20 years old. The number of visits to office-based dermatologists was 33.8 million, and the number of visits to office-based physicians for skin rash was 11.5 million.
According to the 2005 National Health Interview Survey, 11% of children younger than 18 years suffered from hay fever in the past 12 months, 12% from respiratory allergies, and 13% from other allergies. Non-Hispanic white children (13%) were more likely to have had respiratory allergies than non-Hispanic black children (10%) or Hispanic children (9%). Children living in the South (15%) were more likely to have had respiratory allergies than those living in the Midwest (11%), Northeast (10%), or West (9%). Children in fair or poor health (34%) were more than three times as likely to have had respiratory allergies as children in excellent health.
The determination of whether a clinical syndrome may have an allergic etiology was studied by the use of allergy skin tests. Introducing an allergen into the skin of an allergic individual resulted in a cutaneous inflammatory reaction within 10 to 20 minutes. The National Health and Nutrition Examination Survey (NHANES) studied skin-test reactivity on a national sample of a noninstitutionalized population. Each participant was skin tested against eight allergens: house dust, alternaria, cat, dog, mixed giant and short ragweed, oak, perennial rye grass, and Bermuda grass.
The prevalence rate of skin-test reactivity to at least one allergen was 20.2%. Among individual allergens, ragweed and rye grass had the highest individual rates of reactivity, with about 10% of the population reacting to each one. The prevalence rate of skin-test reactivity was higher in males (22.2%) than in females (18.4%). The prevalence rate was higher in blacks (23.2%) than in whites (19.5%), but the difference was not significant. Peak reactivity to at least one allergen occurred in people ages 18 to 24 years. The peak reactivities were 33.3% for males and 25.2% for females.
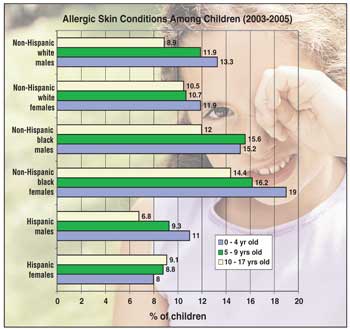
The graph shows that non-Hispanic black females 17 years and younger had the highest prevalence of allergic skin conditions, followed by their male counterparts and non-Hispanic white males. The prevalence of allergic skin conditions varied between boys and girls depending on race. Among non-Hispanic whites, the prevalence of allergic skin conditions was higher among girls four years or younger, but the prevalence rates reversed among children 5 to 17 years old; girls had a higher prevalence rate than boys in the same age group. Among the non-Hispanic blacks, however, the girls had a higher rate of prevalence than that of their male counterparts across all the age groups for children.
To comment on this article, contact editor@uspharmacist.com.


