US Pharm.
2007;32(3):82-88.
Oral lesions afflict children and adults,
and the pharmacist may be the first point of contact regarding treatment. The
prevalence of many oral lesions depends significantly on individual
characteristics. Thus, prevalence rates should be based on studies of general
populations and be stratified by risk factors for the specific lesion. These
factors include sex, age, race/ethnicity, tobacco use, and use of removable
dentures. According to the most current data available, the National Health
and Nutrition Examination Survey (NHANES), 1988-1994, about 28.24% of an adult
group present with oral lesions.1
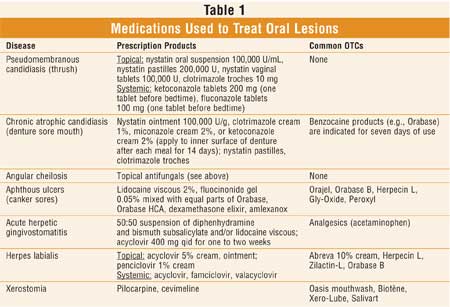
Pharmacists should be
cognizant of common oral lesions and the various medications used for their
management (see Table 1). Oral lesions may present as a multitude of
different diagnoses, ranging from benign to malignant. This article reviews
several oral lesions and conditions, including traumatic/irritational lesions,
candidiasis, primary and recurrent herpes infection, recurrent aphthous
ulcers, lichen planus, leukoplakia, erythroplakia, mucocele, and xerostomia.
Traumatic/Irritational
Lesions
Differential
diagnosis of white lesions depends on whether the lesion can be rubbed off
when wiped with a piece of gauze. A white plaque-like lesion found in an area
of irritation may be an aspirin burn due to "sucking" on an aspirin tablet or
may be irritational keratosis due to constant irritation from a dental
appliance (e.g., denture, orthodontic wire) or biting. Although these lesions
do not rub off, they are not considered malignant. Treatment consists of
removing the irritation. If the lesion does not disappear in a few months, the
patient should be referred to a dental specialist.
A fibroma usually appears as a
submucosal, smooth, pink nodule on the lateral border of the tongue, buccal
mucosa, or lower lip where there is chronic irritation from biting or
friction. These lesions are asymptomatic and do not have a malignant etiology.
Management comprises monitoring and surgical excision.
A mucocele develops when a
minor salivary gland duct in the inner part of the lip (usually lower lip) is
severed and the secretions spill into the tissues. Clinically, it appears as a
swelling that is bluish or the normal pink color of the mucosa. Its size may
increase or decrease over time. These lesions should be monitored and can be
surgically excised.
Candidiasis
Oral candidiasis
can exhibit a variety of clinical patterns and is predominately caused by an
overgrowth of the Candida species, the most common being Candida
albicans, which is part of the normal flora.2 Incidence varies
by age and certain predisposing factors, such as HIV infection, smoking,
dentures, chemotherapy, diabetes, corticosteroid therapy, xero stomia (dry
mouth), and short- or chronic-term broad-spectrum antibiotic use.3,4
Acute pseudomembranous
candidiasis, or thrush, is the most common form of oral candidiasis,
presenting as white, creamy, elevated plaques that easily rub off with gauze,
leaving a painful, raw, ulcerated surface. The most typical sites include
buccal mucosa, dorsal tongue, and palate. Diagnosis is usually based on the
clinical appearance, with or without confirmation by smear or culture of
Candida, because no chairside test (in the office, not sent to the
laboratory) exists for oral candidiasis.5
Topical antifungals (e.g., ny
statin or clotrimazole) are the drugs of choice for uncomplicated, localized
thrush in patients with normal immune function. Systemic antifungals are
usually indicated in cases of disseminated disease and/or in immunocompromised
patients. It is important for patients to continue the drug at least two days
after lesions resolve. If patients use a corticosteroid inhaler, they should
be instructed to brush their teeth and rinse their mouth after every use.
Acidophilus or yogurt is recommended to take with broad-spectrum antibiotics
to reduce the incidence of candidiasis infection.
Chronic atrophic
(erythematous) candidiasis, or denture sore mouth, appears as a red patch or
velvet-textured plaque on the hard palate under a denture (Figure 1).
The most common causes are poor denture hygiene and continuous wear of the
denture.6 The patient should be instructed to clean the denture on
a daily basis and not to wear it while sleeping.7 Topical
antifungal creams or ointments can be applied to the inner lining of the
denture. Additionally, nystatin pastilles or clotrim azole troches may be
used.

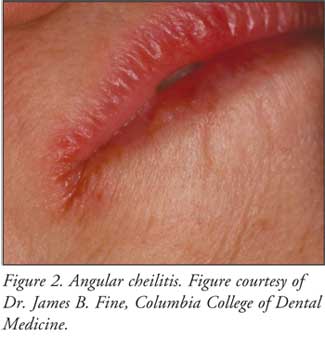
Angular cheilitis, another
form of candidiasis, ranges from slight erythema, with superficial scaling
fissures at the corners of the mouth, to intensely red and ulcerated lesions,
accompanied by soreness and a burning sensation (Figure 2).8
The etiology is multifactorial and includes C. albicans and
Staphylococcus aureus infection, as well as a deficiency of vitamin
B and folic acid.9 Topical antifungal creams and ointments are the
treatment of choice.
Leukoplakia and
Erythroplakia
Since the oral
cavity is composed of many different types of tissues, benign or malignant
neoplasms may occur. According to the World Health Organization, leukoplakia
is defined as "a white patch or plaque that cannot be characterized clinically
or pathologically as any other disease."10 Erythroplakia has
the same definition except that it is a red patch. Speckled leukoplakia is a
combination of red and white lesions.
The primary risk factor for
oral cancer is tobacco use.11 Heavy alcohol consumption (more than
four drinks per day) is a higher synergistic risk factor when combined with
heavy tobacco use.12 Pharmacists should immediately refer patients
to an oral surgeon or otolaryngologist if they have any red or white patches
in the mouth.
Lichen Planus
Lichen planus is a
common dermatosis that occurs on the skin and oral mucosa. About 50% of
patients who have oral lesions also present with skin lesions.13
The tongue and buccal mucosa are the most frequent sites.
Among the different forms of
lichen planus, the reticular form is the most common and appears as slightly
elevated, fine, white lines called Wickham's striae, which have a
lace-like pattern. The etiology of lichen planus is not clear; however, it
does involve an immunologically induced degeneration of the superficial
epithelium.
Treatment for lichen planus,
such as topical corticosteroids (e.g., fluocinonide) and/or corticosteroid
mouthwashes, is usually initiated if lesions are symptomatic.
Ulcerations
Recurrent minor
aphthous stomatitis, typically referred to as canker sores, is the most common
recurrent lesion in the mouth, with a higher incidence in females. Although
the etiology of minor aphthous ulcers is essentially unknown, hypersensitivity
to streptococcal antigens, stress, and hormonal changes have been proposed.
14-16 Aphthous stomatitis is not a viral infection, and it is not
infectious; however, a genetic predisposition maybe present.17
Additionally, patients should be evaluated for vitamin B12 or folic
acid deficiency.18
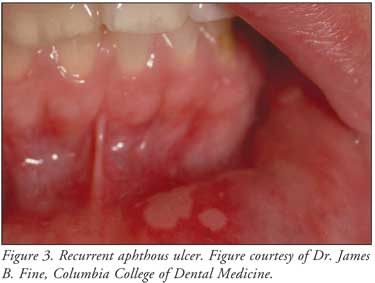
Clinically, aphthous ulcers
first appear as a papule, not a vesicle, on movable mucosa only (e.g., inner
lower lip, lateral border of the tongue, soft palate). The ulcerations are
usually round with a depressed center and a red margin (Figure 3). If
there are several, they do not coalesce. They may be painful, especially when
speaking and eating. The lesions usually heal in about seven to 10 days, but
recurrence is common. It is rare to have lymphadenopathy or fever associated
with these lesions.
In most cases, the natural
history of aphthous ulcers is one of eventual remission. Treatment is usually
palliative and supportive in patients with significant discomfort. Relief of
pain and reduction of ulcer duration are the main goals of therapy.
Medications include topical corticosteroids, analgesics, and antimicrobials.
Topical corticosteroids (e.g.,
Kenalog in Orabase, Orabase HCA) are the mainstays of treatment but only
reduce the pain, not the rate of recurrence.16 Topical analgesics,
including Orabase B (benzocaine) and viscous lidocaine 2%, provide pain
relief. Amlexanox (Aphthasol) 5% paste, an inhibitor of the formation and
release of inflammatory mediators from mast cells and neutrophils, is applied
no more than four times daily and may increase healing and decrease pain but
does not reduce the frequency of recurrent ulcer episodes.
Limited randomized, controlled
studies support the use of tetracycline. One 250-mg capsule was dissolved in
180 mL of water, and the patient was instructed to rinse four times per day
for about five days. Another option is to rinse with 5 mL of tetracycline
syrup 250 mg/5 mL four times daily for five days.
Chlorhexidine gluconate, an
antimicrobial oral rinse, may reduce the severity and pain but not the
frequency of recurrence. In addition, immune modulators such as thalidomide
are used to treat recurrent aphthous ulcers in HIV-infected patients. These
ulcers often have protracted healing times.
Alternative therapies without
scientific evidence include zinc lozenges (one lozenge four to six times
daily), vitamin C (500 mg four times daily), and vitamin B complex (one tablet
four times daily).
Vesicular Lesions
Oral Herpes
Simplex Virus Infection:
Herpes simplex virus (HSV), a DNA virus, is usually classified by anatomical
location. HSV-1 infections, termed herpes labialis, cold sores, or fever
blisters, are located above the torso and are typically associated with oral
lesions. HSV-2 infections, termed herpes genitalia, are located below the
torso and are usually linked to genital lesions. However, in about 30% of
cases, HSV-1 can cause genital herpes by oral-genital or genital-genital
contact with a person infected with HSV-1.
Primary Herpetic
Gingivostomatitis:
The initial HSV-1 outbreak usually occurs in childhood when the virus is
transmitted through such activities as kissing an infected person or drinking
from the same cup of a person with open lesions. The peak incidence of primary
HSV-1 is predominately between two to three years of age, although adults can
also be diagnosed with this disease. The patient usually presents with fever,
headache, lymphadenopathy, malaise, sore throat, and nausea and vomiting.
Later, small vesicles appear in the mouth; they eventually rupture, leaving
small painful ulcers covered by yellow-gray membranes.19 In
addition, there is generalized acute gingivitis.
Treatment of primary acute
herpetic gingivostomatitis in healthy children and adults, including fluids
and acetaminophen, remains palliative. Early treatment with acyclovir may
shorten the duration of all clinical manifestations and infectivity of
affected children.20 Antibiotics are used only to prevent secondary
infection.
Recurrent Intraoral
Herpes/Herpes Labialis:
After primary exposure, this virus remains dormant in the trigeminal ganglion
until a later date when it is reactivated. Recurrences are thought to be due
to stress, sunlight, fever, HIV infection, certain foods, menstruation, trauma
(e.g., after a dental procedure), or other irritants.21 The primary
infection is more severe than recurrent infections. Although not everyone
develops recurrent infections, some may have many recurrences per year.
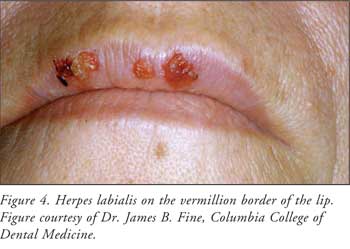
Prodromal symptoms of mild tingling, burning, or itching may occur during the
12 to 36 hours preceding vesicle eruption. The vesicles develop into ulcers,
which finally crust and then heal within 24 to 48 hours (Figure 4).
Spontaneous healing occurs over seven to 10 days. Ulcers are found primarily
on nonmovable mucosa (e.g., lateral border of the tongue and gingival,
perioral, and vermillion border of the lips). These lesions are referred to as
herpes labialis, cold sores, or fever blisters.22
Treatment consists of
controlling symptoms and shortening the duration of active infection. Lesions
are usually mild and self-limited. Topical antiviral and analgesic agents can
help decrease healing time and pain. Acyclovir 5% is an accepted standard
topical therapy.23,24 Systemic antiviral agents, such as acyclovir,
valacyclovir, and famciclovir, may reduce the duration of symptoms but are
helpful only for prodromal symptoms.23 These agents are not
curative, but they may lessen the severity and duration of infection and rate
of recurrence. Since this is a viral infection, antibiotics should not be
used. Corticosteroids have not been effective in treating herpes.
Docosanol (Abreva) 10% topical
cream inhibits fusion of the virus with the human cell membrane, blocking
entry and subsequent viral replication. It is designed to speed healing time
of recurrent oral/facial herpes, and it stopped progression to the blister
stage in about 34% of patients who apply it at the early sign of an outbreak
(redness). This OTC medication should be applied five times per day until the
infection is healed.
Xerostomia:
Xerostomia can be due to medications (e.g., antipsychotics, anticholinergics,
antihistamines, diuretics), illness (e.g., HIV or cancer), or aging. Salivary
glands receive sympathetic and cholinergic innervation. Activation of either
autonomic system will increase secretions, but the cholinergic activation is
the more important system. Anticholinergic drugs bind to the cholinergic
(muscarinic) receptors, thus inhibiting salivary secretions from the salivary
glands, resulting in dry mouth.
Treatment is aimed at
increasing secretions or moisturizing the mouth. Saliva substitutes, or
artificial saliva, have the necessary ions, buffering properties, and
lubricating mucins. OTC products include Oasis, Biotène, Optimoist, Xero-Lube,
and Salivart. Dentists or physicians may prescribe cholinergic drugs, such as
Salagen (pilocarpine) and Evoxac (cevimeline).
Pharmacist's Advice to Patients
Oral lesions can be benign or
malignant; referral to a dentist or an otolaryngologist is appropriate if any
lesion persists for more than two weeks. The pharmacist should review the
patient's history and discuss the clinical appearance of the oral lesion,
including color, location, appearance (raised or flat), and duration. The
pharmacist should assess the patient's condition carefully, as there may be
underlying systemic causes for an innocuous lesion. For benign lesions, such
as aphthous ulcers or herpes labialis, the pharmacist can recommend many OTC
products that may help alleviate pain.
References
1. Shulman JD, Beach MM, Rivera-Hidalgo F. The prevalence of oral mucosal lesions in U.S. adults: data from the Third National Health and Nutrition Examination Survey, 1988-1994. J Am Dent Assoc. 2004;135:1279-1286.
2. Fotos PG, Vincent SD, Hellstein JW. Oral candidosis. Clinical, historical and therapeutic features of 100 cases. Oral Sug Oral Med Oral Pathol. 1992;74:41-49.
3. Akpan A, Morgan R. Oral candidiasis. Postgraduate Med J. 2002;78:455-459.
4. Seelig MS. Mechanism by which antibiotics increase the incidence and severity of candidiasis and later the immunological defenses. Bacteriol Rev. 1966;30:442-459.
5. Heaton ML, Al-Hashimi I, Plemons J, Rees T. Experimental chairside test for the rapid diagnosis of oropharyngeal candidiasis. Compendium. 2006;27:364-370.
6. Golecka M, Oldakowska-Jedynak U, Mierzwinska-Nastalska E, et al. Candida-associated denture stomatitis in patients after immunosuppression therapy. Transplant Proc. 2006;38:155-156.
7. Kanli A, Demirel F, Sezgin Y. Oral candidosis, denture cleanliness and hygiene habits in an elderly population. Aging Clin Exp Res. 2005;17:502-507.
8. Ohman SC, Dahlen G, Moller A, Ohman A. Angular cheilitis: a clinical and microbial study. J Oral Pathol . 1986;15:213-217.
9. Maloney WJ. An overview of angular cheilitis. Bulletin of the 9th District Dental Society. 2001;85:16-17.
10. Dimitroulis G, Avery BS. Biology of oral cancer. In: Dimitroulis G, Avery BS, eds. Oral Cancer: a Synopsis of Pathology and Management. Oxford, England: Wright; 1998:10-25.
11. American Cancer Society: Cancer Facts and Figures 2006. Atlanta, GA: American Cancer Society; 2006.
12. Choi SY, Kahyo H. Effect of cigarette smoking and alcohol consumption in the aetiology of cancer of the oral cavity, pharynx and larynx. Int J Epidemiol. 1991;20:878-885.
13. Weinberg MA, Insler MS, Campen RB. Mucocutaneous features of autoimmune blistering diseases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;84:517-534.
14. Akintoye SO, Greenberg MS. Recurrent aphthous stomatitis. Dent Clin North Am. 2005;49:31-47, vii-viii.
15. ADA Division of Communications. For the dental patient. Canker sores and cold sores. J Am Dent Assoc. 2005;136:415.
16. Jurge S, Kuffer R, Scully C, Porter SR. Mucosal disease series. Number VI. Recurrent aphthous stomatitis. Oral Dis. 2006;12:1-21.
17. Porter S, Scully C. Aphthous ulcers (recurrent). Clin Evid. 2005;13:1687-1697.
18. Volkov I, Rudoy I, Abu-Rabia U, et al. Case report: recurrent aphthous stomatitis responds to vitamin B12 treatment. Can Fam Physician. 2005;51:844-845.
19. Amir J. Primary herpetic gingivostomatitis-- clinical aspects and antiviral treatment. Harefusah . 2002;141:81-84, 124.
20. Kolokotronis A, Doumas S. Herpes simplex virus infection, with particular reference to the progression and complications of primary herpetic gingivostomatitis. Clin Microbiol Infect . 2006;12:202-211.
21. Reznik DA. Oral manifestastions of HIV disease. Top HIV Med. 2005;13:143-148.
22. Arduino PG, Porter SR. Oral and perioral herpes simplex virus type 1 (HSV-1) infection: review of its management. Oral Dis. 2006;12:254-370.
23. Worrall G. Herpes labialis. Clin Evid. 2004;12:2312-2320.
24. Birek C, Ficarra G. The
diagnosis and management of oral herpes simplex infection. Curr Infect Dis
Rep. 2006;8:181-188.
To comment on this article, contact
editor@uspharmacist.com.



